
PPE dehydration in dental professionals is becoming a widespread health concern, especially as dental teams continue to work in high-heat, high-stress environments. Since returning to clinical settings, many dental healthcare providers have reported dehydration-related symptoms including fatigue, difficulty concentrating, and more severe health events like blackouts and emergency room visits.
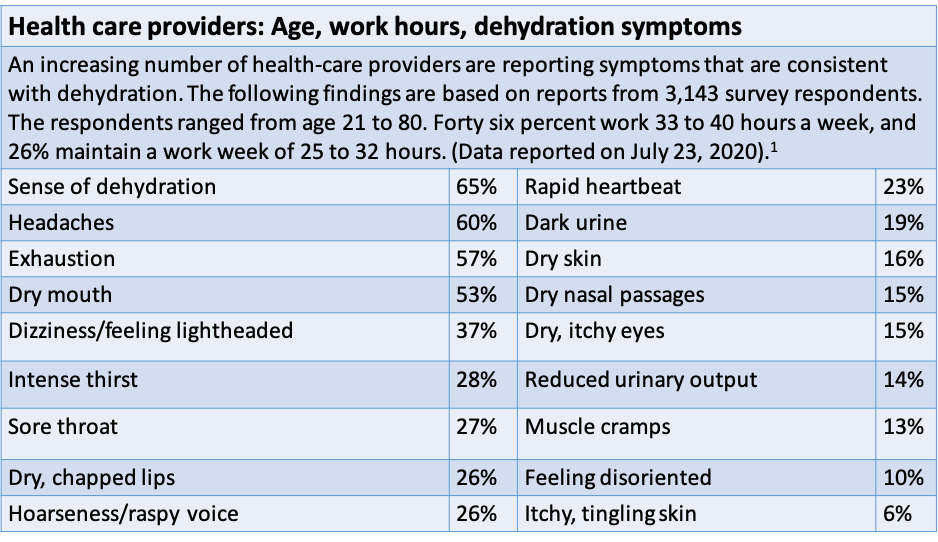
A recent study showed that 65% of dental and healthcare professionals returning to work experienced dehydration—making it the most common symptom among more than 3,000 participants. These numbers highlight the urgent need to address PPE dehydration in dental professionals across all clinical environments.
Why Hydration Is Critical in Dental Settings
The human body is made up of 60% water. Even small drops in hydration affect critical organs:
-
Brain and heart: 73% water
-
Lungs: 83%
-
Skin: 64%
Dehydration happens when more fluid is lost than consumed, disrupting core functions. The result? Fatigue, dizziness, memory lapses, and long-term complications involving the kidneys, blood pressure, and brain function.
How PPE Contributes to Dehydration in Dental Professionals
Wearing multiple layers of PPE is now routine in dental practices. This protective gear traps heat and restricts airflow. A recent survey found:
-
27% wear a respirator and surgical mask
-
26% wear a surgical mask and face shield
-
56% wear all three: respirator, surgical mask, and face shield
This layering significantly increases body heat and sweat output. To make things worse:
-
62% of dental professionals only remove PPE at lunch
-
7% keep it on for their entire shift
This discourages hydration and bathroom breaks—especially in environments where removing PPE is discouraged or time-consuming.
Hidden Year-Round Risks of PPE Dehydration in Dental Professionals
Many assume dehydration is a summer-only concern, but indoor environments pose year-round risks:
-
Air conditioning and heating systems dry the air
-
Fans accelerate evaporation, speeding fluid loss
-
Dust, allergens, and low humidity make breathing more difficult
-
Stress and anxiety reduce salivary flow, further dehydrating the body
All of these factors compound the issue of PPE dehydration in dental professionals, regardless of the season.
Practical Hydration Strategies for Dental Professionals
Since the body’s thirst response lags behind actual dehydration, it’s important to hydrate before symptoms occur.
Recommended hydration habits:
-
Drink water before, during, and after shifts
-
Avoid sports and energy drinks with high sugar, caffeine, or acidity
-
Choose:
-
Plain water
-
Herbal iced teas (xylitol-sweetened if needed)
-
Water-rich foods like cucumber, melons, and yogurt
-
What to avoid:
-
High-sodium snacks
-
Processed foods
-
Skipping hydration to stay “productive”
A low-sodium diet and scheduled hydration breaks can go a long way toward maintaining performance and well-being.
Make Hydration a Non-Negotiable Part of Dental Practice
PPE dehydration in dental professionals is not just a workplace inconvenience—it’s a serious occupational hazard. Ensuring consistent hydration should be viewed as a clinical standard, not a personal option.
Dental professionals must make hydration and bathroom breaks part of their protected workflow. Failing to address these risks doesn’t just harm individuals—it affects patient care, team performance, and overall safety.
Disclaimer: This article provides general information and is not a substitute for medical advice. Always consult a licensed medical professional regarding any health concerns.
Link to CDC’s official page on Heat Stress in Healthcare Settings
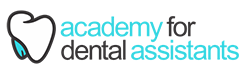
Summary of the physiological consequences of acute mild hypohydration in healthy humansWatso JC, Farquhar WB. Hydration status and cardiovascular function. Nutrients. 2019 Aug 11;11(8):1866. doi: 10.3390/nu11081866. Used under CC BY 4.0.